- med4vl
- Nov 9, 2021
- 1 min read
top of page
Select blog
- med4vl
- Nov 8, 2021
- 4 min read
Updated: Jun 6, 2022
Important Concepts in the Evaluation of Unconjugated Hyperbilirubinemia
Introduction
The workup of unconjugated hyperbilirubinemia in the neonate is quite complex and can be frustrating to learn. But once you comprehend the rationale for each investigation, you will be able to grasp contempary algorithms with less difficulty. It is the aim of this lecture to help you organize vital information in your mind so that you may be better prepared to conceptualize the strategic approach to evaluating these patients. Now, because algorithms can vary depending on location, when necessary, please be sure to refer to local guidelines.
Please note that this is not an all-encompossing lecture on neonatal jaundice. The evaluation of conjugated hyperbilirubnemia, in particular, necessitates a different approach altogether, which for the sake of brevity will NOT be discussed during here.
Before considering investigations, remember that it is important take a careful history and perform a thorough physical examination, which may reveal risk factors for the development of severe hyperbilirubinemia or provide a hint as to the underlying mechanism.
Example:

Investigations
When it has been determined that we are dealing with an unconjugated hyperbilirubinemia, there are five or six tests that are commonly ordered:
Antiglobulin test (a.k.a., Coomb’s test)
Complete blood count
Reticulocyte count
Peripheral blood smear
Blood type and RH status
Other testes (e.g., especially G6PD assay) may also be warranted. These tests are not necessarily ordered all at once, but altogether the combined results of these investigations will help narrow down the differential diagnosis.

Differential Diagnosis
Hemolytic Disease of the Newborn
Hemolytic disease of the newborn occurs when there is incompatibility between maternal and fetal blood types, most commonly ABO incompatibility and rhesus isoimmunization. This aetiology can be identified with a positive direct or indirect Coomb’s test. The other tests have usually already been ordered, which could reveal a decreased hemoglobin level, reticulocytosis, and microspherocytosis; these findings are suggestive, but are not pathognomonic. The presence off spherocytes, in particular, is transient and will diminish over time, unlike with hereditary spherocytosis where it will persist.
RBC Enzymopathy and Membranopathy
Two intrinsic causes of hemolysis include red blood cell enzymopathy and membranopathy. Both could cause a decreased hemoglobin level and reticulocytosis, just as with hemolytic disease of the newborn, however the Coomb’s test will be negative. As well, with RBC membranopathy there are abnormal findings on the peripheral blood smear (e.g., spherocytes or elliptocytes). Certain tests can then be used to confirm a specific condition. For example, the EMA binding test can confirm the diagnosis of hereditary spherocytosis.

With erythrocyte enzyme defects, red cell morphology could yield nonspecific findings. For example, with G6PD deficiency the peripheral blood smear may reveal bite and blister cells. More definitively, specific enzyme assays can confirm the diagnosis of G6PD deficiency and other enzymopathies as well (e.g., pyruvate kinase deficiency).
Hemoglobinopathies may also occur, but are a less common cause of intrinsic hemolysis.
Polycythemia
Polycythemia is associated with elevated hemoglobin, and these infants are often plethoric on the physical examination. A few potential etiologies to consider include twin-twin transfusion, maternal-fetal transfusion, delayed cord clamping, and macrosomia in infants of diabetic mothers.

Blood Extravasation and Sepsis
Signification extravasation of blood can occur with extensive bruising or sequestration of blood within a closed space (e.g., cephalohematoma). Investigative studies may not reveal specific findings, but physical examination could point you in the right direction. At times, however, the location of blood extravasation can be less conspicuous, as may be the case with adrenal or subdural hemorrhage.
Lab findings can be highly variable with infections in the neonatal age group. Because of the possibility of severe morbidity and even mortality, there is a low threshold for further evaluation and management.
Decreased bilirubin clearance, increased enterhepatic circulation, and/or other factors
This last section includes a myriad of disease entities. The common factor between them is that with the exception of hyperbilirubinemia, these initial aforementioned lab tests are unrevealing. I’ve grouped them all together because after ordering this initial battery of tests you will have likely excluded a hemolytic disease process, and can now either diagnose a benign entity or continue investigating for a pathologic entity. Determination of the etiology requires deduction based on findings from the history and physical examination, and if necessary, further testing. Decreased bilirubin clearance, increased enterhepatic circulation, and/or other factors may underlie the indirect hyperbilirubinia in these patients.
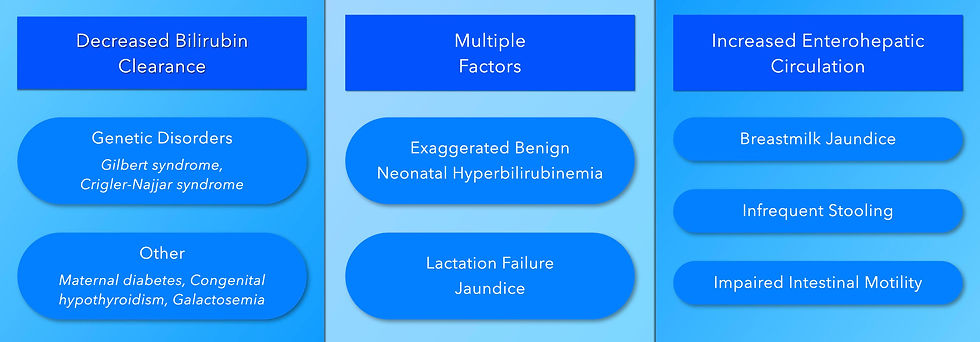
The first three etiologies to consider are breast milk jaundice, lactation failure jaundice, and exaggerated benign neonatal hyperbilirubinemia (a.k.a. physiologic jaundice). There can be quite a bit of overlap between these conditions, but the history and physical examination may help to distinguish between them. For example, the infant with breastmilk jaundice usually presents after the 4th day of life and will be thriving; while the infant with lactation failure jaundice typically presents in the first week of life – but not during the first 24 hours – and may be dehydrated with weight loss due to insufficient caloric and fluid intake. With benign neonatal hyperbilirubinemia, an exagerated and prolonged course of physiologic jaundice may occcur in babies with risk factors (e.g., low birth weight).
Decreased bilirubin clearance can occur due to a few different genetic disorders (e.g., Gilbert syndrome and Crigler-Najjar syndrome); where there is suspicion genetic testing can be used to confirm the diagnosis. A few other conditions may also decrease the clearance of bilirubin (e.g., maternal diabetes, congenital hypothyroidism, galactosemia); and additional testing is based on supporting findings (e.g., thyroid function testing for hypothyroidism, erythrocyte galactose uridyl transferase activity for galactosaemia).
Impaired intestinal motility, infrequent stooling, and potentially breastmilk jaundice can result in increased enterhepatic circulation of bilirubin.
Conclusion
When the etiology is not clear following history, physical examination, and these basic lab tests, then further workup may be required. For example, an enzyme assay may help elucidate the diagnosis when red cell morphology is normal, coombs test is negative, but the reticulocyte count is high. When infection is suspected, then a septic screen is paramount. But for the most part, these few tests along with a skilfully taken history and physical will lead to an accurate diagnosis in the vast majority of cases. I hope that this very brief lecture helped clarify a topic that – for me at least- is very complicated. If you would like more information on specific disease entities (e.g., lactation failure jaundice) or other related topics, look for other lectures here on our YouTube channel, Medical Education for Visual Learners.
Recommended Reading
Pan, Debra H.; Rivas, Yolanda (2017). Jaundice: Newborn to Age 2 Months. Pediatrics in Review, 38(11), 499–510. doi:10.1542/pir.2015-0132
American Academy of Pediatrics Subcommittee on Hyperbilirubinemia. Management of hyperbilirubinemia in the newborn infant 35 or more weeks of gestation. Pediatrics 2004; 114:297.
Video Lecture
- med4vl
- Aug 16, 2021
- 1 min read
Updated: Nov 29, 2021
Chest X-ray Findings
Consolidation
The presence of fluid density material within the right middle lobe results in a wedge-shaped opacity in the right lower zone adjacent to the heart. Note the superior border of the opacity is sharply demarcated at the level of the horizontal fissure.

Air Bronchograms
Another finding, that is a little more difficult to appreciate, is the presence of air bronchograms. Air filled bronchi that are surrounded by alveolar infiltrates can appear as dark, radiolucent branching columns within the area of opacification.

Silhouette Sign
Consolidation of the right middle lobe results in effacement of the right heart border; obscuring the interface between the lung and heart. This is referred to as the silhouette sign.

Also note that the superior border of the right hemidiaphragm is clearly defined. This helps to differentiate a right middle lobe pneumonia from a right lower lobe pneumonia, in which case the right hemidiaphragm would be obscured.

Normal/Increased Lung Volume
Unless there is coinciding atelectasisi, there usually is no loss of lung volume.
Pitfalls
Radiographic evidence of often pneumonia worsens during the first few days of treatment and can take several weeks to completely resolve.
Video Lectures
bottom of page